Clinical standards for establishing facial balance and harmony in lingual orthodontics
üčResults
|
 |
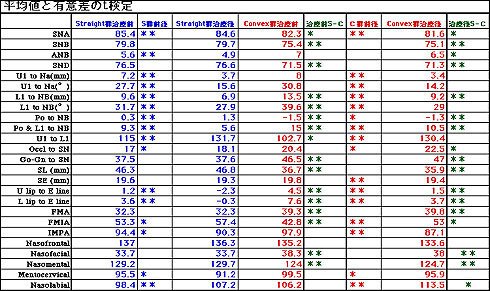 |
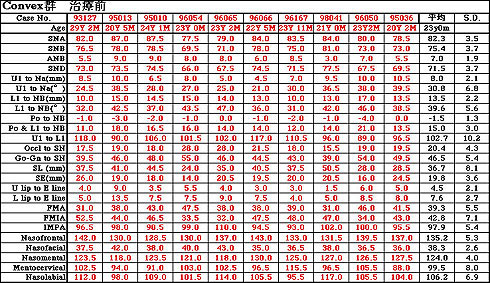
1: The pre-treatment lateral cephalograms of S Group showed significantly larger SNA, SNB, SND, Po to NB, U1 to L1, SL, FMIA and nasomental values, and significantly smaller L1 to NB, Po and L1 to NB, Go-Gn to SN, upper and lower lip to E line, FMA, and nasofacial values.
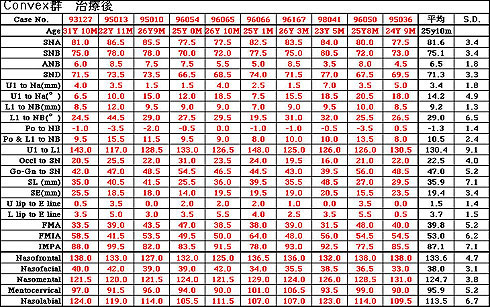
2: After treatment, S Groups exhibited significantly larger SNA, SNB, SND, Po to NB, SL, FMIA and nasomental values, and significantly smaller ANB, L1 to NB, Po and L1 to NB, occlusal plane to SN, Go-Gn to SN, upper and lower lip to E line, FMA, nasofacial, and nasolabial values.
3: Comparison of the before and after records revealed an SNA reduction as a skeletal change as well as dento-alveolar changes including uprighting of U1 and L1, increases in occlusal plane to SN and nasolabial angle, and a decrease in mentocervical angle in both S Group and C Group. An ANB reduction was noted only in S Group. |
üčDiscussion
Female patients with an Angle Class II malocclusion or bimaxillary protrusion were divided into two groups, one with and the other without satisfactory profile improvement.
Skeletal changes: The subjects in C Group clearly had a more retrognathic mandible. Before and after comparison showed an SNA reduction but not an SNB increase in either group, suggesting a difficulty of achieving skeletal improvement by growth or counter-clockwise rotation of the mandible to move B point forward in adult orthodontics.
In other words, the ANB improvement obtained in adult orthodontics seemed to be mainly due to lingual movement of the upper anterior teeth and associated distal movement of A point. Vertically, the subjects in C Group were severe high angle (dolichofacial) cases with significant differences in Go-Gn to SN and FMA between the two groups. |
üčDiscussion-2
However, there was no change in Go-Gn to SN or FMA with treatment in either group, indicating adequate vertical control without clockwise rotation of the mandible during treatment.
From these results, it seemed that good anchorage preparation is required prior to the use of Class II elastics for Class II improvement in order to prevent bowing effects, and that sufficient vertical control measures should be included in the treatment plan.
Dento-alveolar changes: The lower anterior teeth were more upright in S Group than C Group both before and after treatment. This may be due to dental compensation of the jaw discrepancy by labial tipping of the lower incisors in C Group with a larger ANB. Generally, upright lower anterior teeth are regarded as essential for Class II correction and long-term stability of the result. |
üčDiscussion-3
The upper anterior teeth were lingually tipped with marked reductions in the distance and angle measurements in C Group. This was also reflected in the marked increase in U1 to L1, suggesting rabitting or lingual tipping of the upper anterior teeth to compensate for the large ANB difference. It may therefore be necessary to avoid excessive lingual tipping of the upper anterior teeth by keeping the interincisal angle within the range of 130 to 136üő. For this purpose, the amount of torque and force applied to the upper anterior teeth during upper anterior retraction should be carefully controlled.
There has been a tendency to emphasize technical aspects due to difficulty of case handling in lingual orthodontics. We felt, however, that there is a need for a new diagnostic system specific to lingual orthodontics as we analyzed the before and after cephalograms of the subjects in an effort to obtain clinical standards for facial balance and harmony. |
üčSummary
1. Importance of vertical control during treatment.
2. The lower anterior teeth should be uprighted while the upper
anterior teeth should be retracted under good torque control in
the treatment of Class II malocclusions.
3. Anchorage preparation of the lower arch should be established to
prevent bowing effects.
4. U1 to L1 should be corrected to around 130 even in severe
high-angle cases to avoid excessive lingual tipping of the upper
anterior teeth.
5. A new diagnostic system specific to lingual orthodontics seems to
be necessary. |
|